CPT 99203 – New Patient Office or Outpatient Visit, 30–44 Minutes
CPT Code 99203 Definition
CPT 99203 describes an office or other outpatient evaluation and management (E/M) visit for a new patient. The service requires a medically appropriate history and/or examination and either:
- Low-level medical decision-making (MDM), or
- 30–44 minutes of qualifying physician or qualified healthcare professional time on the date of the encounter.
Related codes for CPT 99203
| Code | MDM | Time |
|---|---|---|
| 99202 | Straightforward | 15–29 minutes |
| 99203 | Low | 30–44 minutes |
| 99204 | Moderate | 45–59 minutes |
| 99205 | High | 60–74 minutes |
Who Can Bill CPT 99203?
CPT 99203 may be reported by physicians and other qualified healthcare professionals authorized to perform and bill outpatient E/M services, subject to scope-of-practice, credentialing, and payer requirements.
The patient must also qualify as new. A patient is not necessarily new because the individual provider has never treated them. Previous professional services from another clinician in the same group, specialty, and subspecialty may establish the patient.
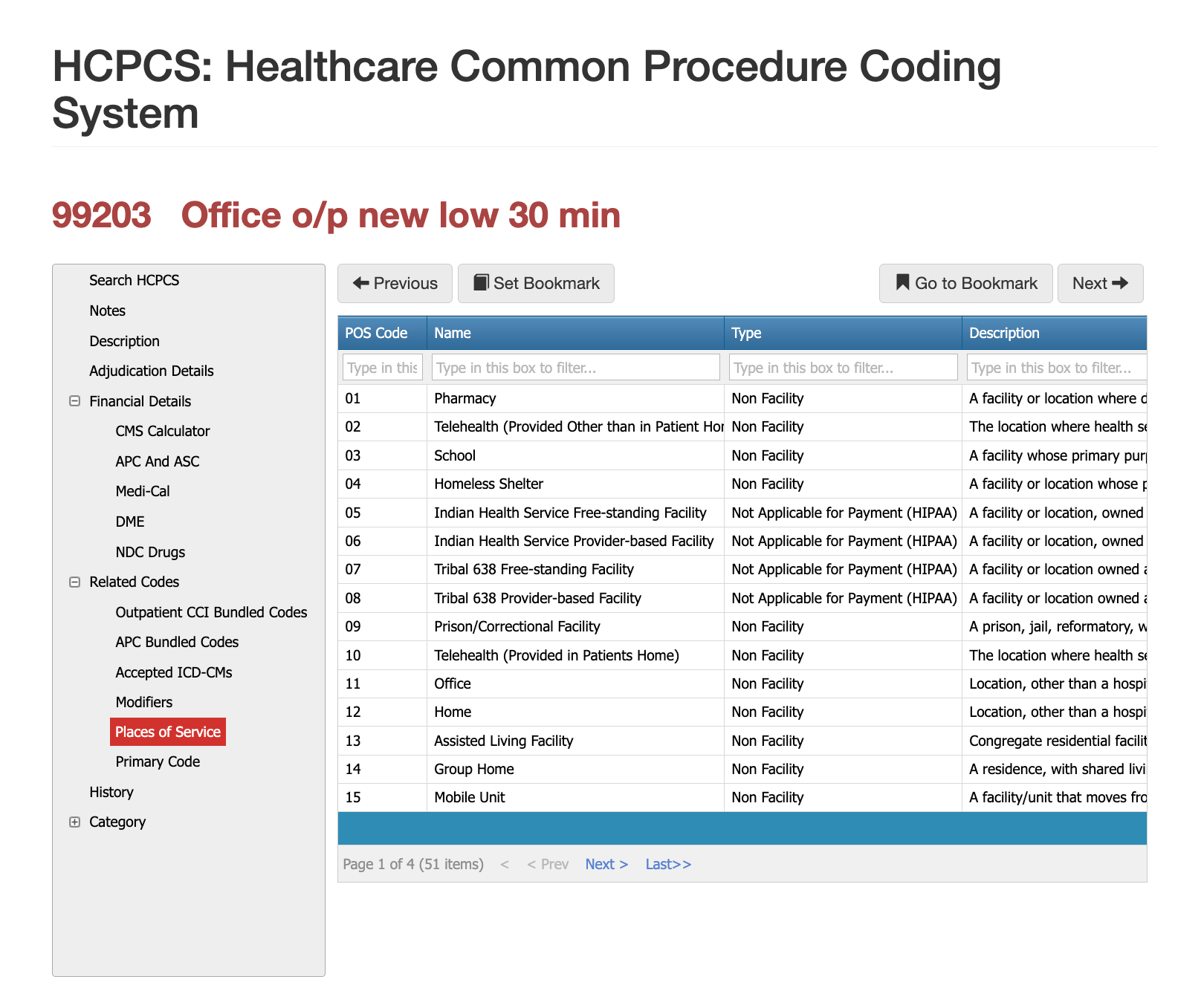
Places of Service for CPT 99203
CPT 99203 may be reported in eligible outpatient settings, including:
- Physician offices
- Urgent care centers
- Retail clinics
- Specialty practices
- Hospital outpatient departments
- Approved telehealth settings
The place of service must reflect the actual encounter. Telehealth claims must follow the payer’s current modifier, modality, consent, and documentation rules.
Medical Decision-Making Requirements
MDM is based on three elements:
- Number and complexity of problems addressed.
- Amount and complexity of data reviewed and analyzed.
- Risk associated with patient management.
CPT 99203 generally requires at least two of these three elements to meet the low level.
Common Diagnoses Reported With CPT 99203
No diagnosis automatically supports CPT 99203. The documentation must independently establish low-level MDM or 30–44 minutes of qualifying time.
- Stable chronic illnesses.
- Acute uncomplicated musculoskeletal injuries.
- Uncomplicated respiratory or ENT conditions.
- Dermatologic complaints.
- Gastrointestinal symptoms.
- Mild behavioral health concerns.
- New symptoms require a limited diagnostic evaluation.
The same diagnosis may support CPT 99202, 99203, or 99204, depending on the work performed and documented.
Problems Addressed: Low-Level MDM
Two or more self-limited or minor problems.
One stable chronic illness.
One acute, uncomplicated illness or injury.
One stable acute illness.
A condition must be evaluated or managed during the encounter. Listing a diagnosis in the history does not establish that it was addressed.
For example, a new patient with controlled hypertension is evaluated, current readings are reviewed, and the existing treatment plan is continued. The stable chronic illness may contribute to low-level MDM.
Data Reviewed and Analyzed
Qualifying data activities may include:
- Reviewing an external clinical note.
- Reviewing the result of a unique test.
- Ordering a unique test.
- Using an independent historian when medically necessary.
The same information cannot be counted repeatedly as separate data elements.
For example, an orthopedic provider reviews an urgent care note, reviews an existing X-ray result, and orders an MRI. These activities may contribute to the data element when properly documented.
Risk of Patient Management
Low risk may include:
- Recommending over-the-counter medication.
- Advising rest, home treatment, or activity modification.
- Ordering routine diagnostic testing.
- Continuing conservative treatment.
Risk is based on management decisions, not on the diagnosis alone. Initiating or adjusting a prescription medication may pose a higher risk depending on the circumstances.
3-Year Rule for New Patient Consults
A patient is generally new if they have not received professional services from a physician—or another physician, or a qualified healthcare professional of the same specialty and subspecialty within the same group—during the previous three years.
For example, a patient saw one cardiologist in that group 18 months ago and now sees another. The patient will generally remain established.
However, a patient treated by an orthopedic physician two years ago may qualify as new when later seeing a dermatologist in the same multispecialty organization, subject to payer requirements.
A patient does not become new solely because:
- A different clinician performs the visit.
- The office location changes.
- The patient was seen only once.
- A different billing identifier is used.
- The record is stored in another system.
- Fewer than three years have passed.
Modifiers for CPT 99203
Several modifiers can be used in conjunction with CPT Code 99203; however, the modifier should be used only when supported by the documentation, services performed, and payer policy.
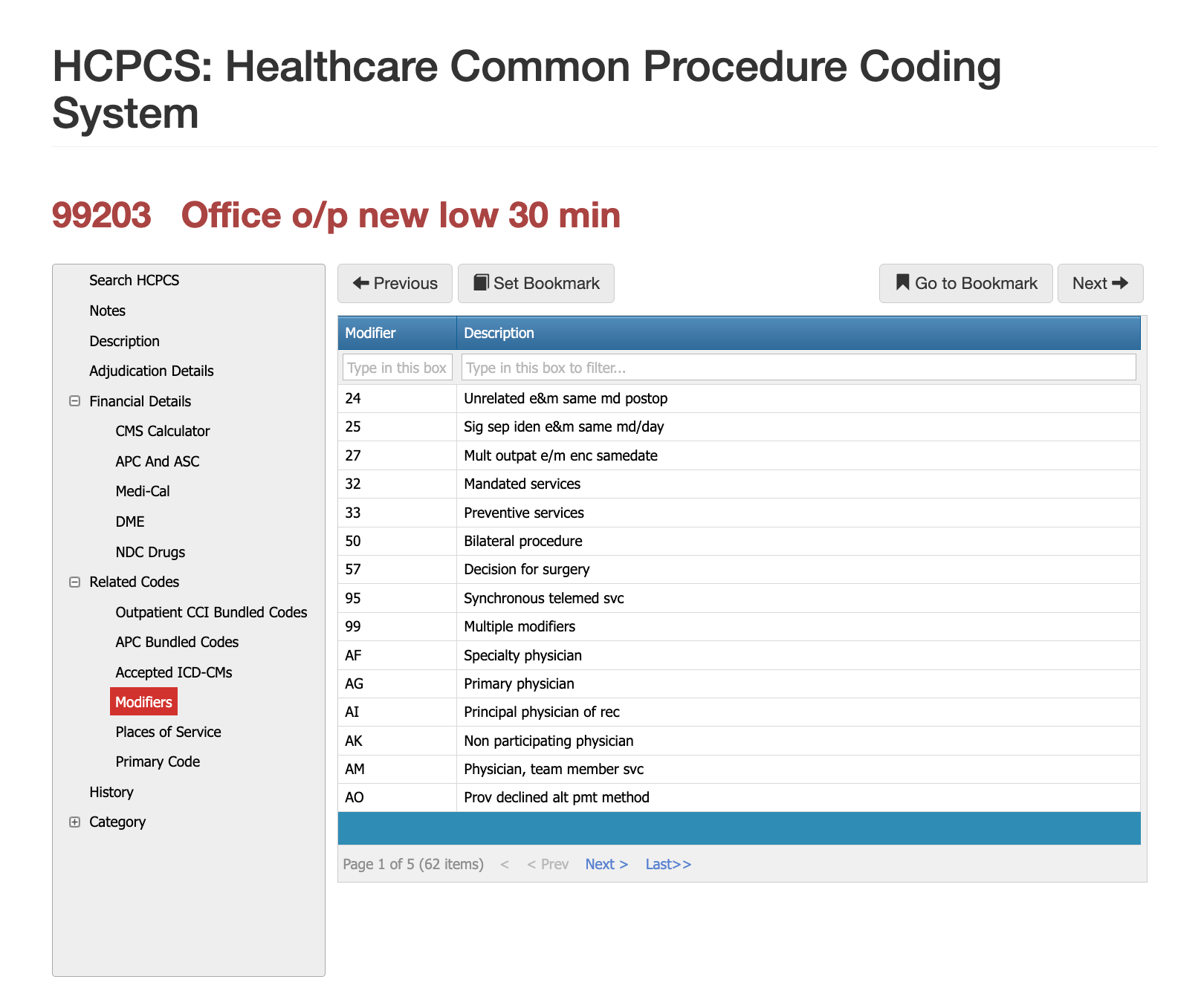
Modifier 25 and CPT 99203
Modifier 25 may be appended when the provider performs a significant, separately identifiable E/M service on the same date as another procedure.
For example, a new patient is evaluated for a skin lesion and also receives a separate evaluation and treatment plan for an unrelated rash. CPT 99203 with modifier 25 may be appropriate when both services are independently supported.
Modifier 25 may be inappropriate when the E/M documentation only reflects the routine evaluation required to perform the procedure.
Modifier 95 & 99203: Synchronous Telemedicine
Modifier 95 may apply when CPT 99203 is performed through real-time interactive telecommunications and permitted by the payer.
Documentation should support the telehealth modality, required consent, provider and patient locations when applicable, and the reported E/M level.
Modifier 33: Preventive Service
Modifier 33 identifies qualifying preventive services. Its use with CPT 99203 is uncommon because CPT 99203 is generally a problem-oriented visit. Preventive counseling during the encounter does not automatically justify modifier 33.
CPT 99203 During a Procedure’s Global Period
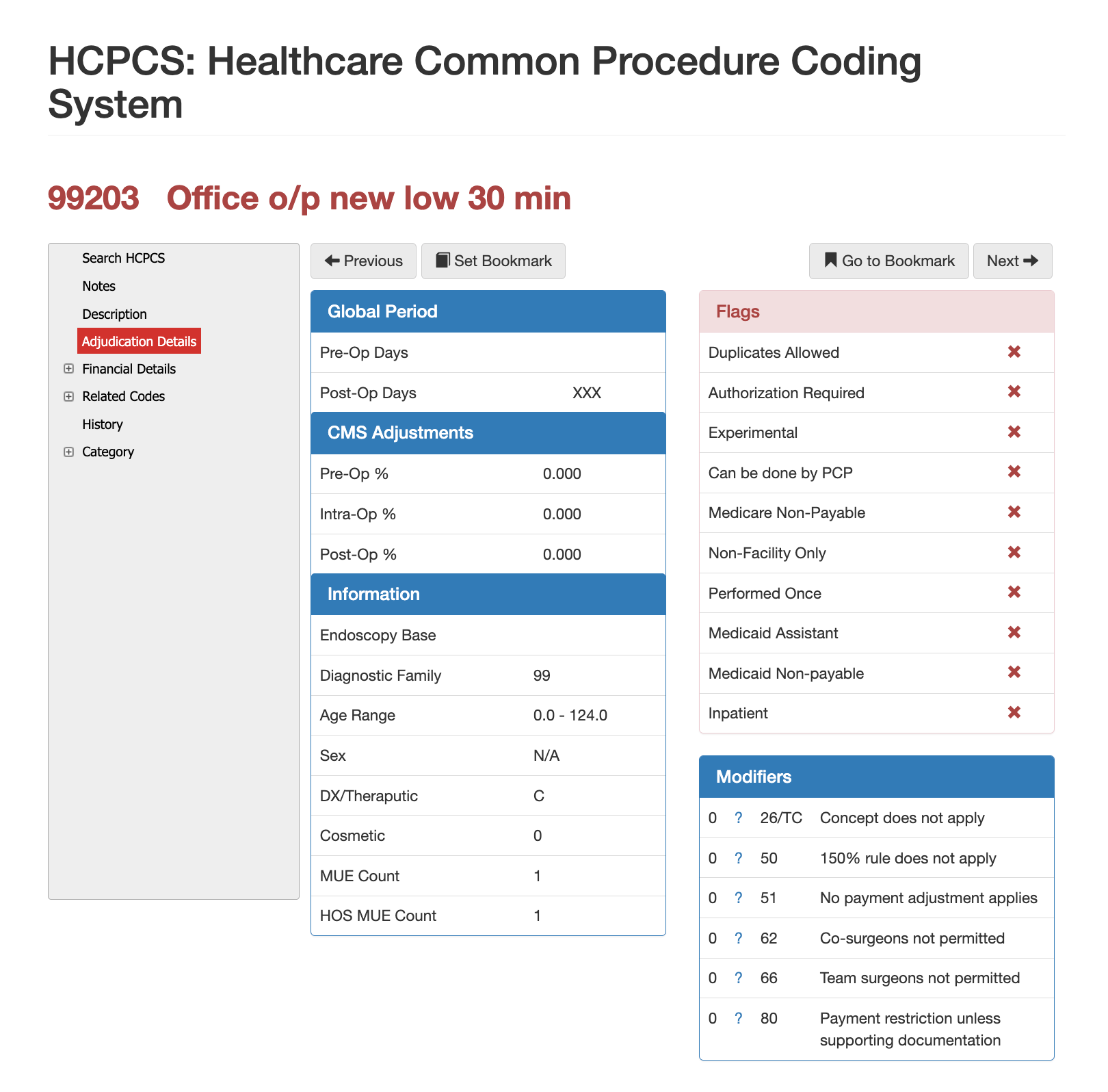
CPT 99203 may be included in a procedure’s global surgical package when the visit relates to routine postoperative care. Medicare commonly assigns 0-, 10-, or 90-day global periods to procedures. During that period, routine follow-up services related to the surgery are generally included in the procedure payment and should not be separately reported with CPT 99203. A separately billable E/M service may be appropriate when it addresses a condition unrelated to the surgery, and all documentation and modifier requirements are met.
For example, a patient returns during the 10-day global period after removal of a skin lesion. A routine wound check is included in the surgical payment and should not be billed separately. If the provider also evaluates a new, unrelated respiratory complaint, an established-patient E/M code with modifier 24 may be appropriate when the service is medically necessary and fully documented.
Most Common Denials for CPT Code 99203
CPT 99203 may be denied, downcoded, or reviewed when:
- The documentation does not support low-level MDM.
- Fewer than two MDM elements meet the low level.
- Total time is missing or below 30 minutes.
- Nonqualifying time is included.
- The patient is established.
- Medical necessity is unsupported.
- Modifier 25 is incorrectly used.
- The place of service is inconsistent.
- Documentation conflicts with the submitted claim.
- Same-day services are improperly bundled or unbundled.
For example, a provider reports CPT 99203 for a minor rash but documents only a brief evaluation and over-the-counter treatment recommendation. Without a qualifying time or sufficient MDM, CPT 99202 may be more appropriate.
Inappropriate Downcoding for CPT 99203
CPT 99203 may also be underreported when billers focus only on the diagnosis or perceived simplicity of the complaint.
For example, a new patient presents with uncomplicated shoulder pain. The provider reviews an outside note and imaging result, orders additional testing, and develops a treatment plan. If at least two MDM elements meet the low level, CPT 99203 may be appropriate even though the diagnosis appears routine.
Billers should code from the complete documentation. Consistently selecting CPT 99202 to avoid scrutiny can reduce reimbursement and distort utilization data.
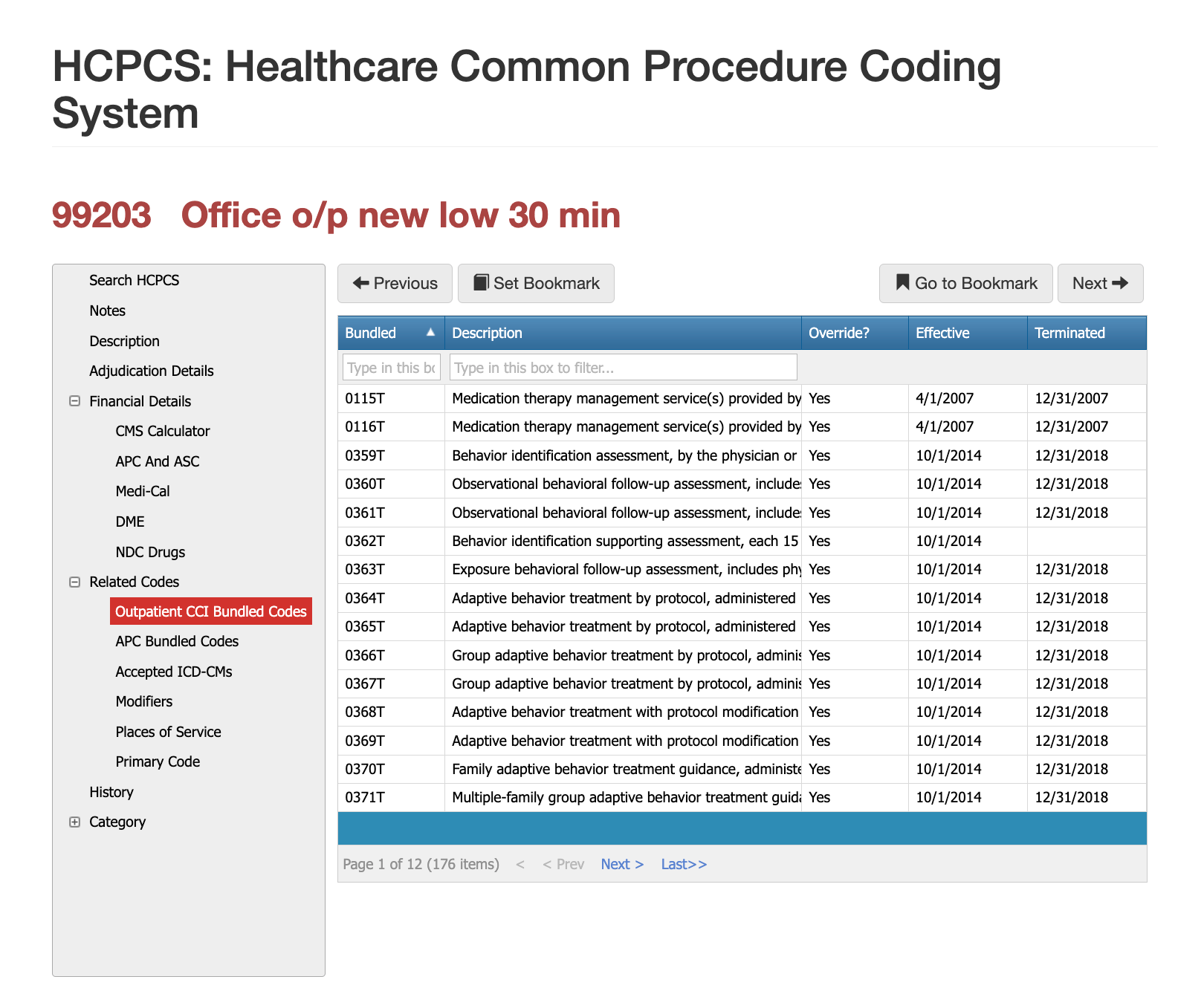
CPT 99203 and Unbundling Risks
Unbundling occurs when a provider separately reports CPT 99203 for evaluation work that is already included in another billed procedure or service. A separate E/M code may only be reported when the documentation supports a significant, medically necessary service beyond the routine assessment required to perform the procedure. Appending modifier 25 does not make an otherwise bundled service separately payable.
For example, a new patient presents for the removal of a superficial foreign body. The provider examines the affected area, confirms that removal is appropriate, performs the procedure, and gives routine aftercare instructions. Billing CPT 99203 in addition to the procedure would likely constitute unbundling because the documented evaluation is integral to the procedure. If the provider also evaluates a separate condition, such as unrelated persistent abdominal pain, CPT 99203 with modifier 25 may be appropriate when the additional E/M work and code level are independently supported.
CPT 99203 Approval and Denial Examples
APPROVAL: MDM
A new patient presents with an uncomplicated ankle injury. The provider reviews external imaging and recommends conservative treatment. The problems and data may support low-level MDM.
APPROVAL: Time
A provider spends 36 qualifying minutes reviewing records, evaluating a new patient, counseling the patient, ordering tests, and documenting the encounter. CPT 99203 may be supported based on time.
DENIAL: Likely CPT 99202
A new patient presents with a minor rash. The provider performs a limited evaluation, reviews no external data, recommends nonprescription treatment, and documents no qualifying time. The record may support straightforward MDM.
DENIAL: Established Patient
A patient saw one family medicine physician in a group 14 months ago and later sees another family medicine physician at another location owned by the same group. The patient is generally established.
DENIAL: Unsupported Modifier 25
A provider evaluates a lesion and performs a procedure. The E/M documentation only reflects the work necessary to perform that procedure. Modifier 25 may be unsupported.
APPROVAL: Modifier 25
During a lesion procedure, the provider separately evaluates an unrelated rash, reviews previous treatment, and prescribes medication. Modifier 25 may be appropriate when the separate E/M service is fully documented.
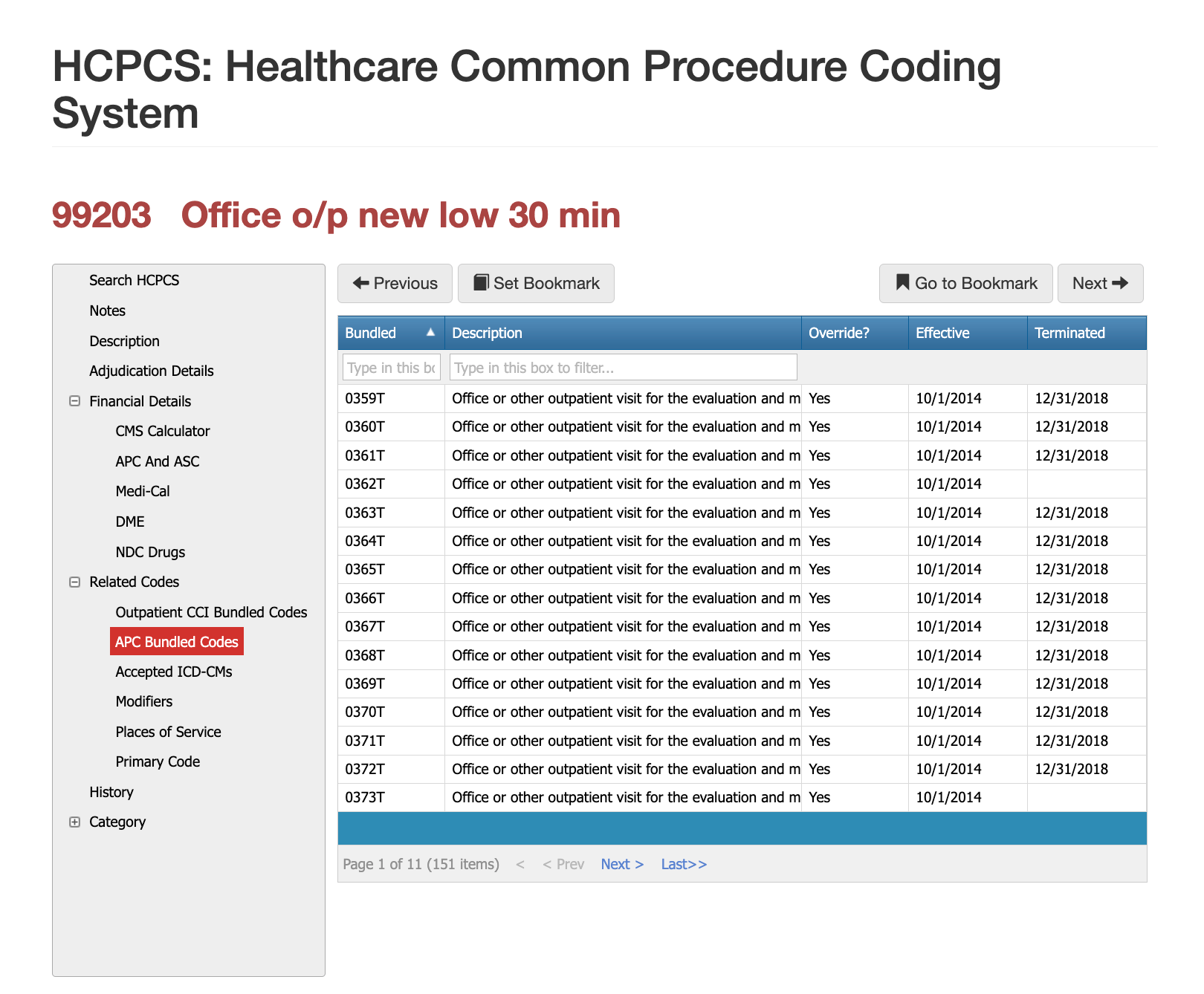
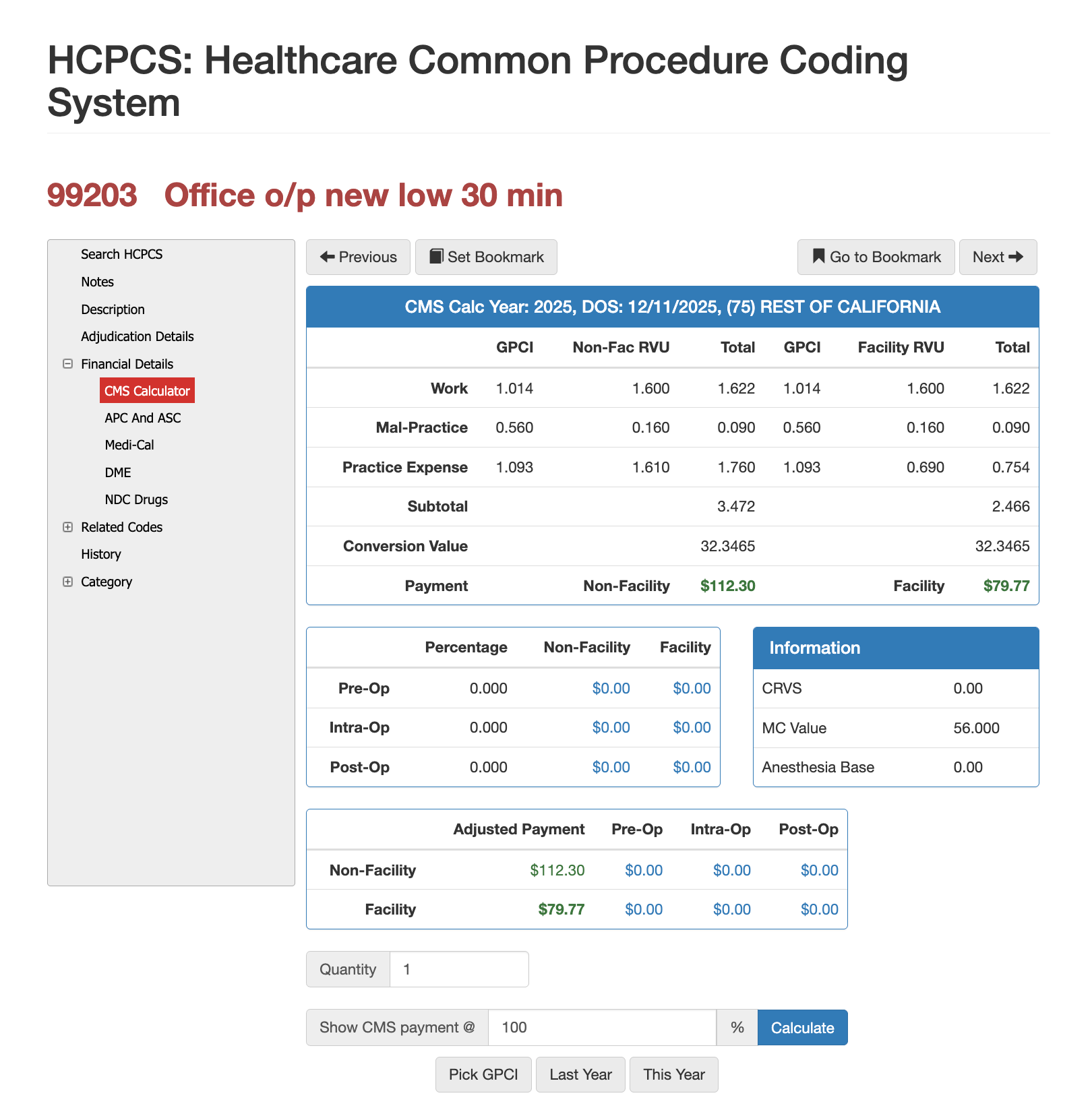
RVUs and Reimbursement for CPT 99203
Payment for CPT 99203 is influenced by physician work, practice expense, and malpractice RVUs. Final reimbursement may vary based on:
- Geographic adjustments.
- Facility or non-facility setting.
- Medicare conversion factors.
- Commercial fee schedules.
- Contracted reimbursement rates.
- Payer policies.
- Modifiers and other billed services.
Provider organizations may evaluate CPT 99203 utilization, payment, denial rates, and adjacent-code reimbursement during contract negotiations.
Health plans may review whether utilization is consistent with the provider's specialty, the patient population, and the documentation. Unusual patterns may justify review, but do not independently establish improper billing.
Virtual AuthTech and iVECoder help payer and provider organizations model reimbursement, compare fee schedules, analyze coding relationships, and evaluate payment outcomes.
Simplify Coding Research
For more than 30 years, PCG Software has supported Health Plans, MSOs, IPAs, TPAs, and provider organizations in improving coding accuracy, strengthening compliance, and reducing fraud, waste, and abuse. Our solutions, including Virtual Examiner®, VEWS™, and iVECoder®, are built on decades of payer-side adjudication experience and reflect the same logic used by health plans nationwide. National regulatory guidance, payer policies, compliance standards, and large-scale claims review patterns inform this CPT 99203 analysis.
Toss out the CPT book.
Stop researching articles.
Sign up for iVECoder today!
About PCG
For more than 30 years, PCG Software has helped health plans, provider organizations, and delegated entities improve coding accuracy, payment integrity, compliance, and fraud, waste, and abuse detection through payer-focused software and claims auditing expertise.
Click to share with others