CPT Code 90471 – Immunization Administration for Vaccines
CPT Code 90471 Guide Summary
Quick Summary: CPT code 90471 is one of the most commonly billed preventive service codes, yet it’s frequently misused, bundled incorrectly, or denied due to sequencing and documentation errors. This code represents the administration of a single vaccine, not the vaccine itself, and is highly sensitive to bundling logic, modifier usage, and payer-specific rules.
What CPT Code 90471 Actually Means
CPT 90471 represents the administration of a single vaccine, regardless of the type, as long as it is delivered via injection such as intramuscular, subcutaneous, or intradermal routes. It does not include the vaccine product itself, only the work associated with administering it.
In simple terms, this code is used when a provider gives a patient one vaccine shot. If additional vaccines are given during the same visit, this code is no longer sufficient on its own and must be sequenced correctly with additional administration codes.
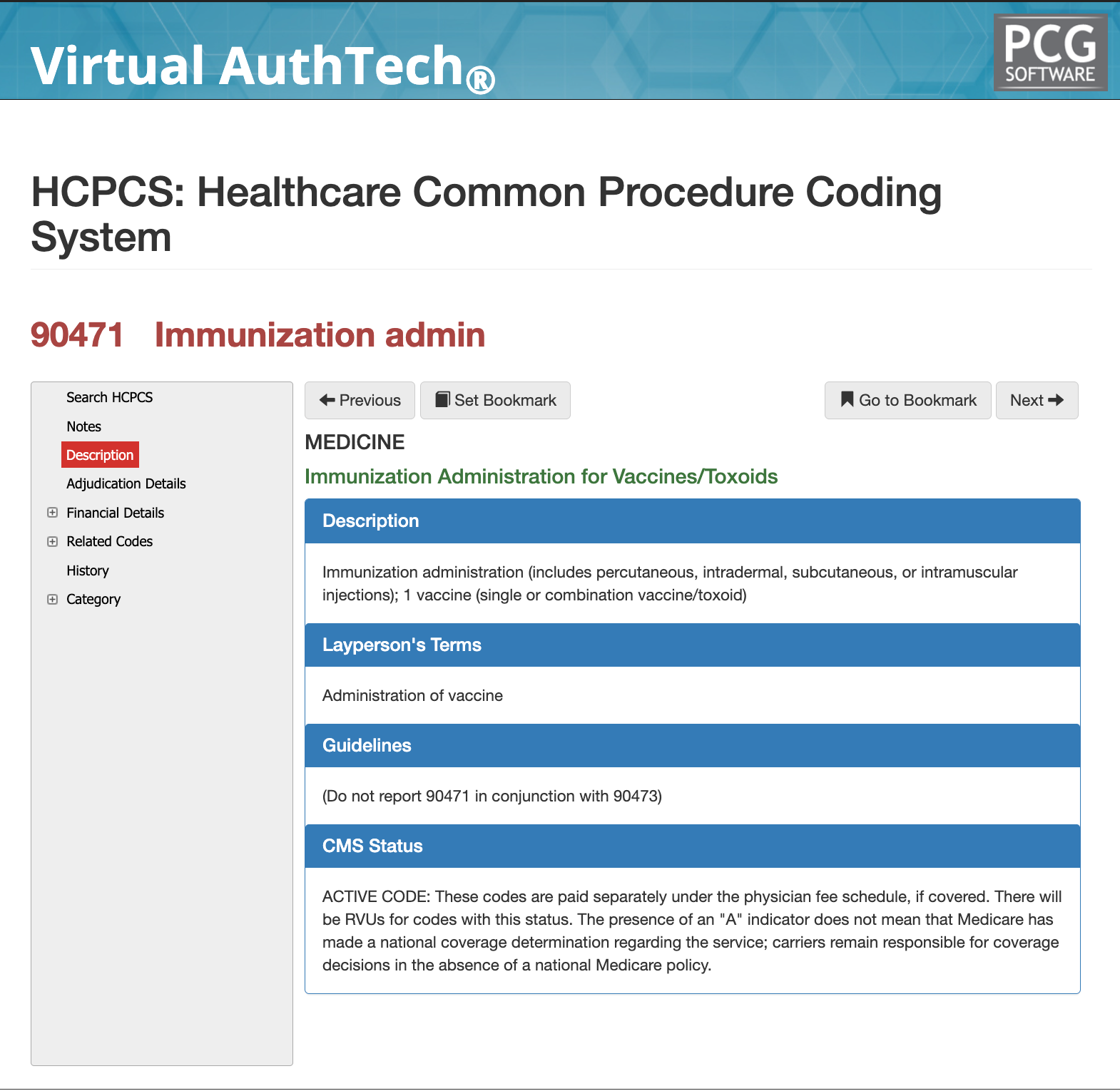
Formal CMS Description for 90470
“Immunization administration (includes percutaneous, intradermal, subcutaneous, or intramuscular injections); 1 vaccine (single or combination vaccine/toxoid)”
Layperson Description for 90471
This code is used when a provider gives a patient a shot (vaccine). It does not include the cost of the vaccine itself—just the act of administering it.
Basics of 90471 cpt code
Choose the right code
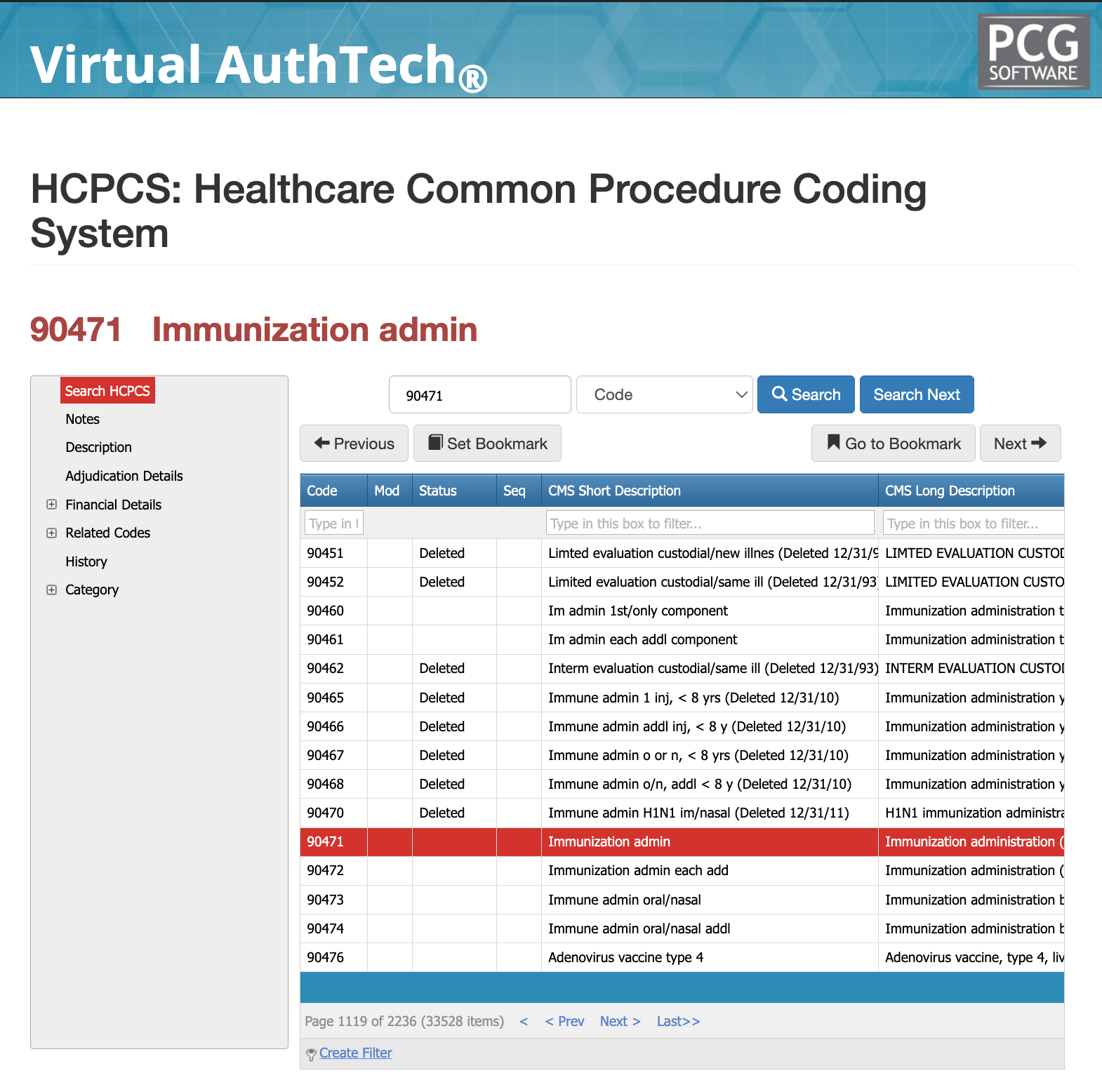
The screenshot from our Virtual AuthTech and iVECoder AI coding solutions learly shows why CPT 90471 must be used instead of older immunization administration codes like 90465–90468, which are explicitly marked as deleted. Continuing to bill deleted codes is not just outdated—it leads to immediate claim denials or silent system substitutions depending on the payer, both of which create compliance risk and inaccurate reimbursement.
CPT 90471 replaced these legacy codes and standardizes how injectable immunizations are reported today. Any system, billing workflow, or provider still referencing the deleted codes in the image is operating on outdated logic and is likely processing claims incorrectly. At scale, this creates consistent payment errors, either through denials that slow revenue or improper adjudication that increases audit exposure.
The key takeaway is simple: if a code is marked deleted, it should never appear on a claim. CPT 90471 exists specifically to replace those codes, and using anything else indicates a breakdown in coding updates, system configuration, or internal compliance controls.
Related Codes and Consideration when paying for or billing for CPT 90471
Applicable Modifiers for CPT Coder 90471
The modifier panel in the images reinforces that CPT 90471 generally does not require modifier usage, and in most cases, adding modifiers is either unnecessary or incorrect.
Common modifiers like 50 (bilateral), 51 (multiple procedures), 62 (co-surgeons), and 66 (team surgeons) are shown as not applicable, which aligns with the fact that immunization administration is a straightforward service without surgical or bilateral components. Modifier 51, for example, should not be used because multiple vaccine administrations are handled through proper code sequencing (90471 + 90472), not modifiers.
Modifier 50 is also inappropriate since vaccines are not bilateral procedures. In rare cases, modifier 80 (assistant surgeon) may appear in systems but requires strong documentation and is typically irrelevant for immunizations. The practical takeaway is that if modifiers are being used with 90471, it usually signals a billing error or misunderstanding, and correct coding should rely on proper code selection and sequencing rather than modifier adjustments.
Bundled Codes for 90471
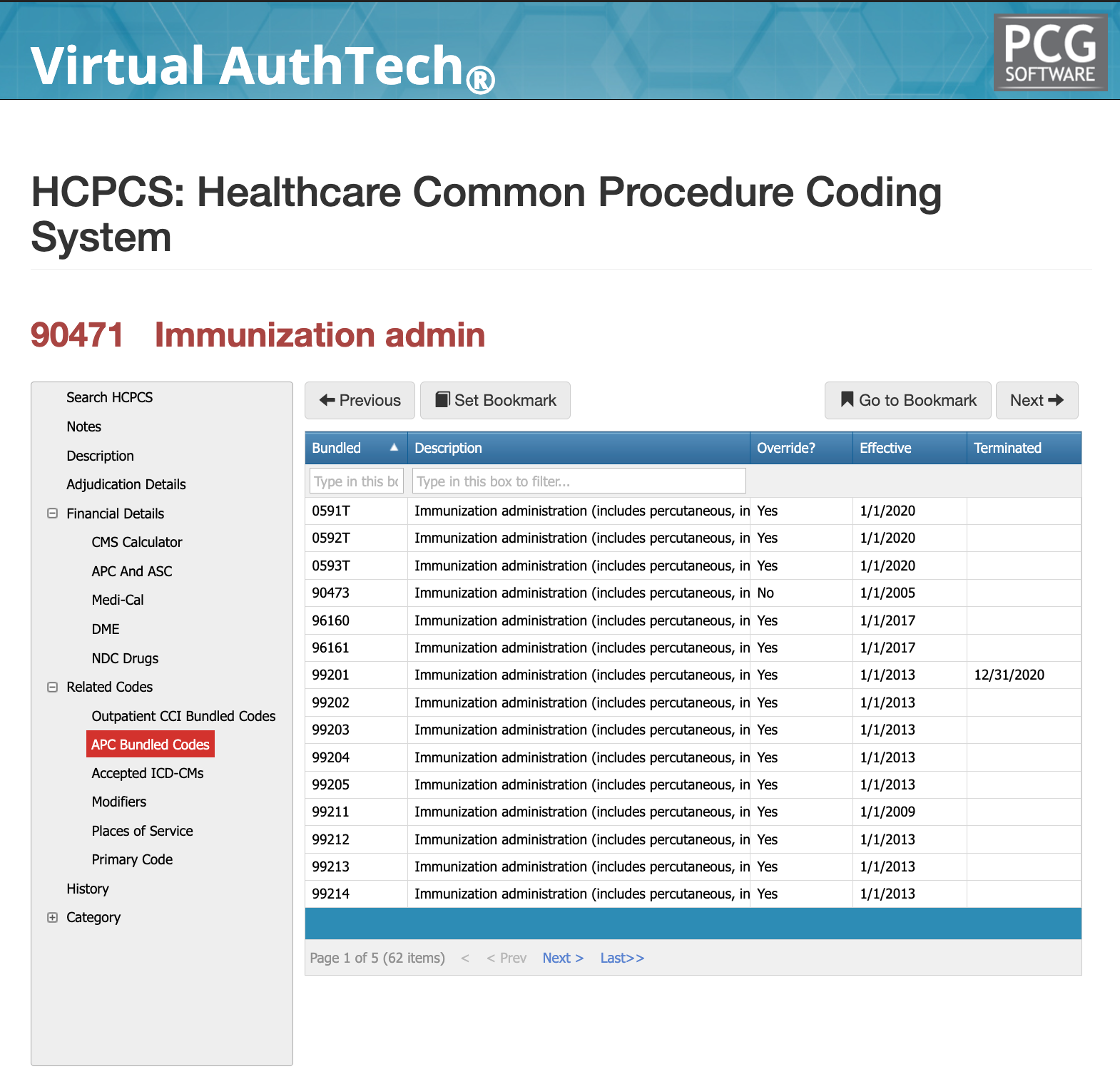
APC Bundled codes for 90471
The APC bundled codes shown in the image highlight that CPT 90471 is frequently evaluated within a broader outpatient payment structure where immunization administration is not always treated as a fully independent reimbursable service. Many of the listed codes—particularly outpatient visit codes like 99201–99205 and 99211–99214—are marked as bundled with override capability, meaning the system may allow separate payment only if proper billing logic and documentation support it. This indicates that 90471 is often packaged alongside evaluation and management services or other outpatient procedures, and reimbursement depends heavily on correct sequencing and clinical justification. If billed incorrectly, the administration may be absorbed into the overall APC payment or reduced, rather than denied outright, making these errors harder to detect but still financially impactful.
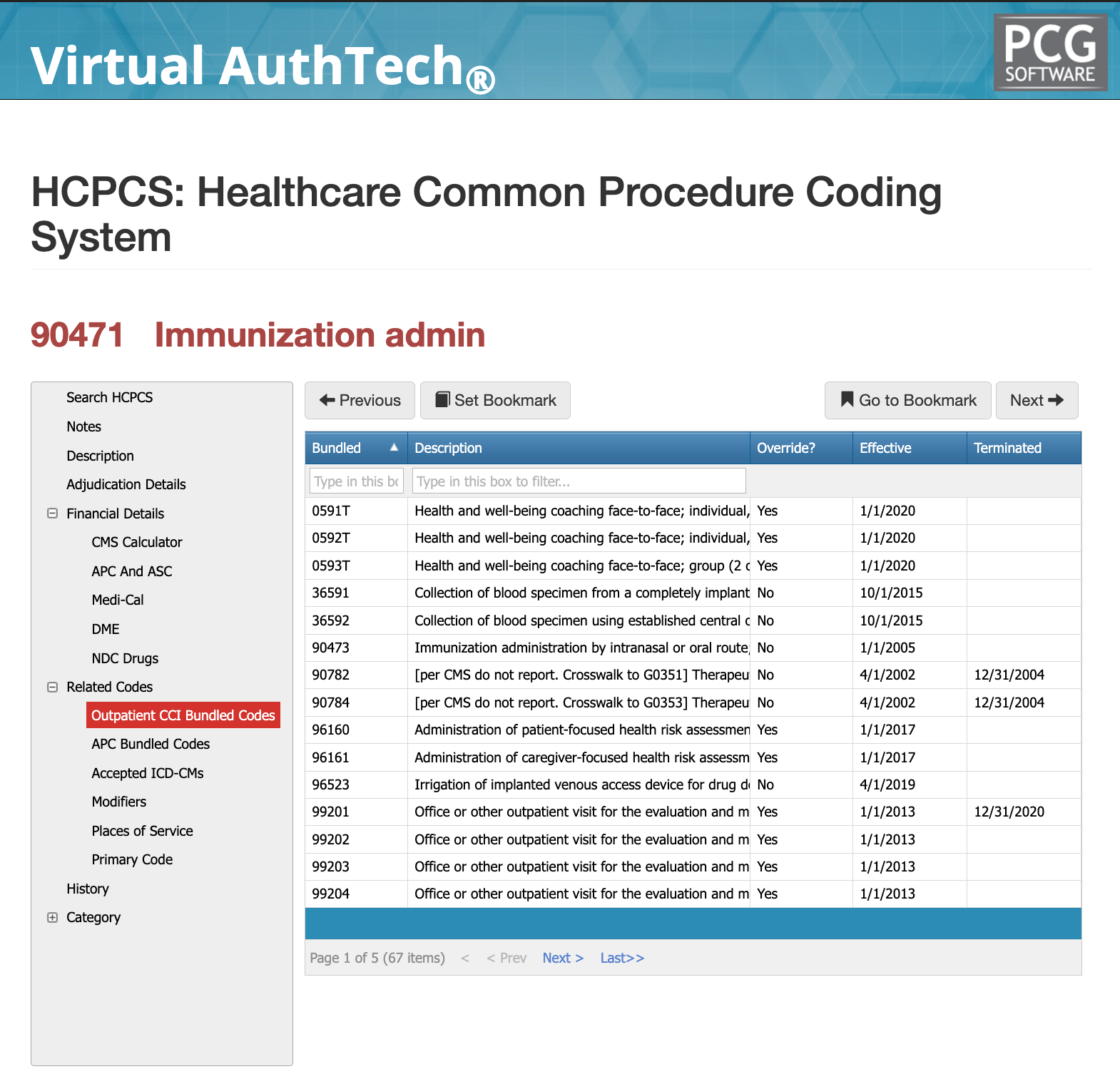
CCI Bundled codes for 90471
The CCI bundled codes shown in the image reflect stricter edit logic where CPT 90471 is evaluated against other procedures to determine if they can be billed together at all, rather than simply adjusted for payment. Several codes, including oral/intranasal administration (90473) and other procedural services, are marked as not overrideable, meaning they cannot be reported with 90471 under any circumstance. Others, such as certain E/M services and assessment codes, allow overrides but only with proper documentation and justification. This indicates that incorrect combinations will typically result in outright denials rather than reduced payment, especially when route conflicts or duplicate administration logic is involved. The key takeaway is that CCI edits enforce billing correctness at the claim level, and misuse of 90471 within these relationships is a primary driver of denials and audit exposure.
Most Commonly Used POS for 90471
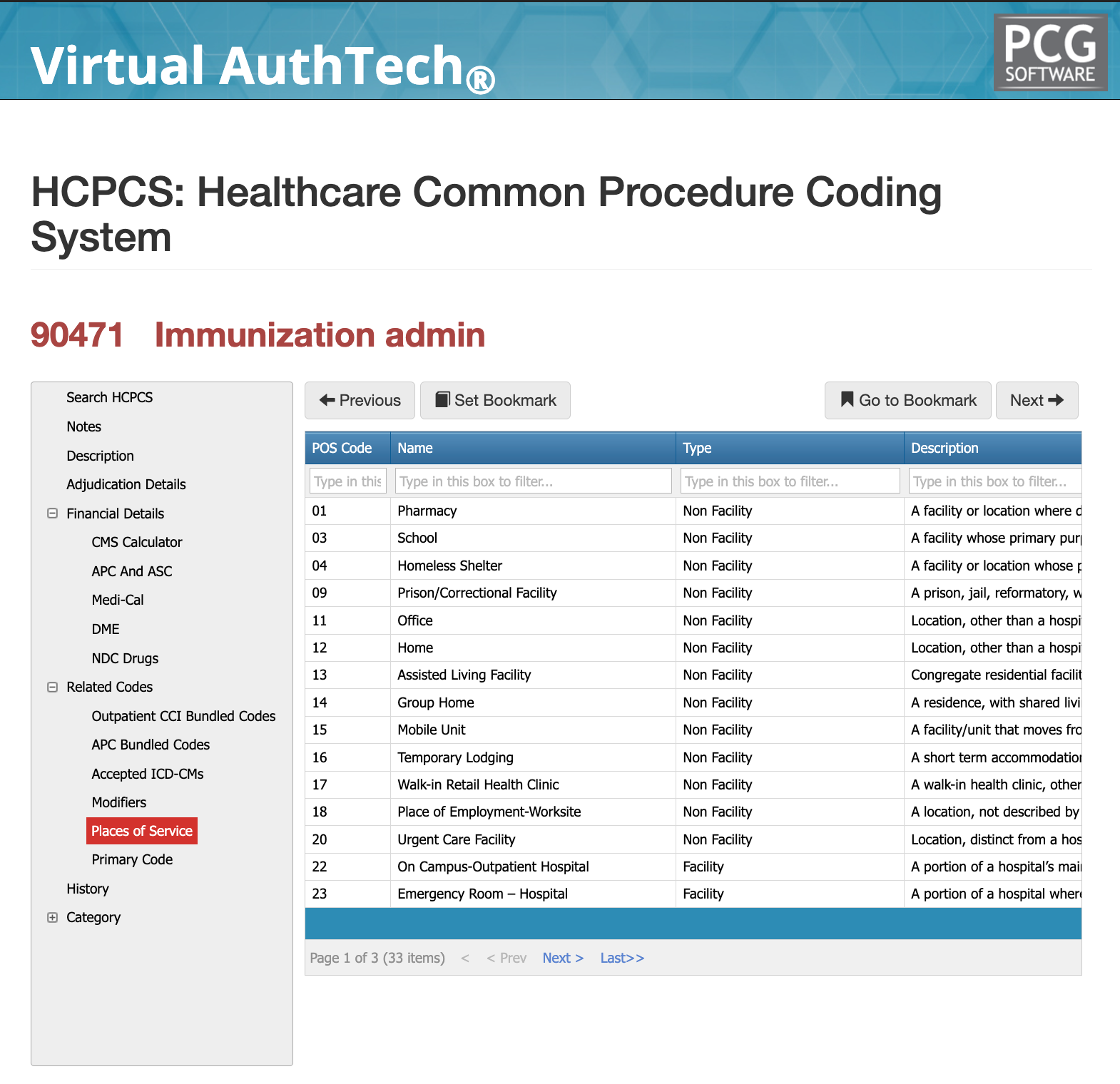
The place of service data reinforces where CPT 90471 is most commonly and appropriately billed, aligning directly with who is administering the vaccine. The image shows that the code is predominantly used in non-facility settings such as offices (POS 11), urgent care centers (POS 20), retail clinics (POS 17), and even pharmacies (POS 01), which matches how immunizations are typically delivered in high-volume outpatient environments. It can also extend into home settings (POS 12) and community-based locations like schools or mobile units, further emphasizing its role in preventive and accessible care. While facility settings such as outpatient hospital departments (POS 22) and emergency rooms (POS 23) are included, they are less common for routine immunizations and introduce different reimbursement dynamics. Overall, the place of service confirms that 90471 is designed for widely distributed, outpatient-driven administration, which is why volume, consistency, and correct sequencing become far more important than complexity in individual claims.
Adjudication and Global Period Considerations
Global Periods 90471
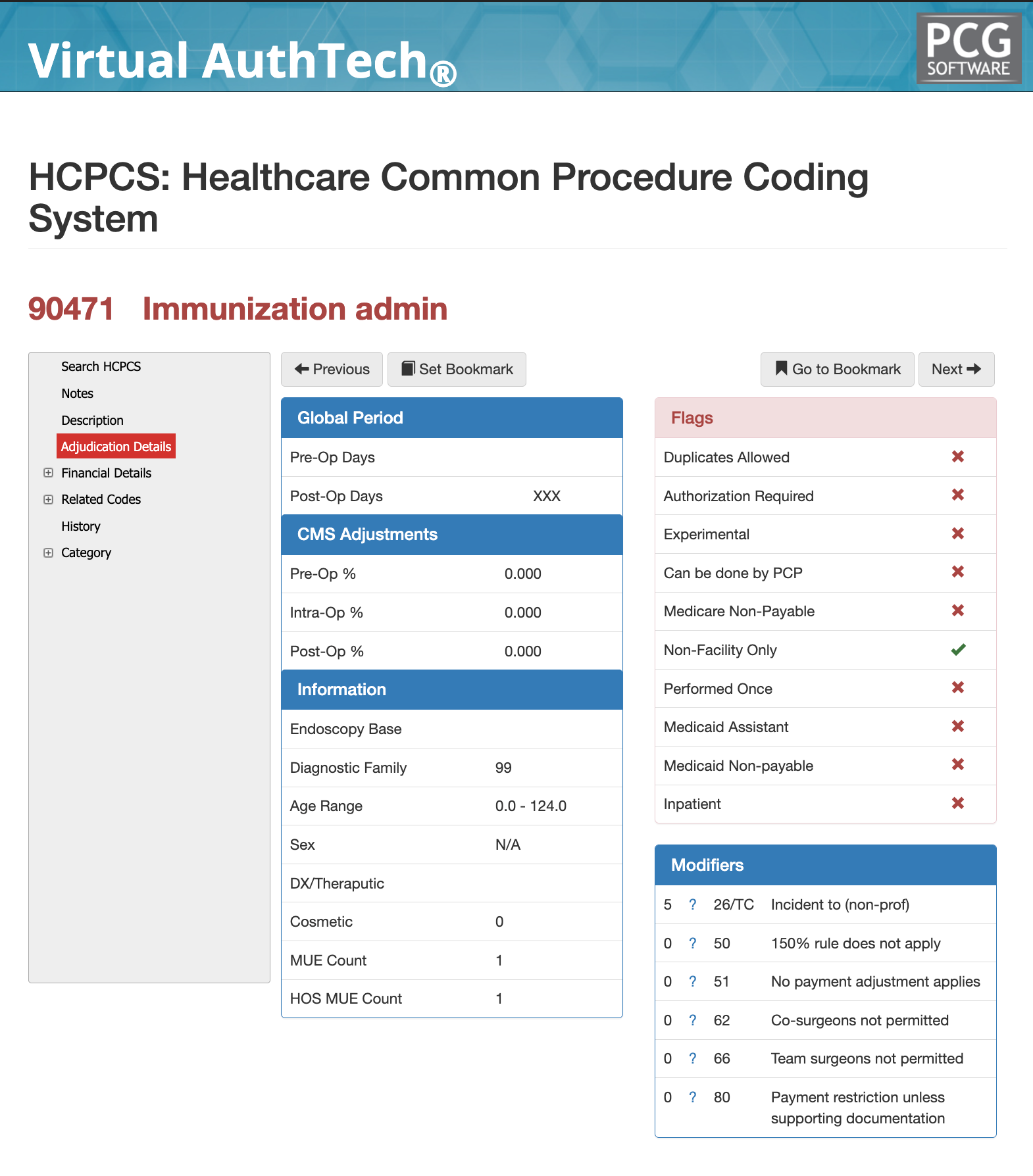
The adjudication details show that CPT 90471 carries no pre-op, intra-op, or post-op global period, meaning it is reimbursed as a standalone service each time it is performed. There are no bundled surgical timelines or percentage reductions applied, and the MUE of 1 reinforces that it is expected to be billed once per encounter as the primary administration code. The flags further confirm this is a non-facility, non-inpatient, non-experimental service with no authorization requirement, which simplifies adjudication but also increases scrutiny on correct code selection and sequencing. In practice, reimbursement is driven less by timing rules and more by correct pairing with vaccine product codes and avoidance of duplicates.
Medi-Cal Logic for CPT Code 90471
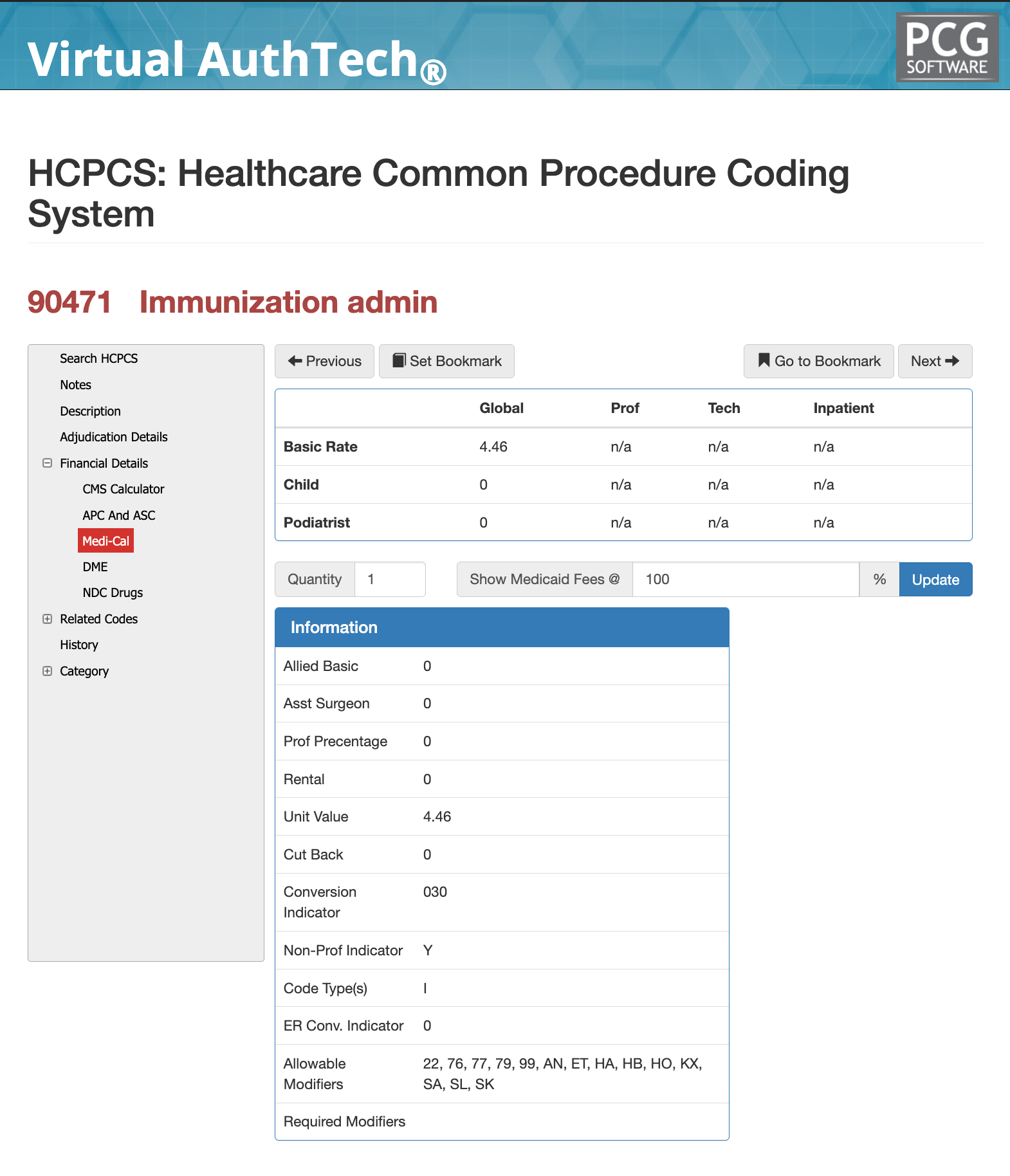
The Medi-Cal view shows a flat unit-based reimbursement structure, with a defined base rate and conversion indicator rather than RVU-driven variability. There are no assistant surgeon, professional split, or inpatient adjustments, reinforcing that 90471 is treated as a simple outpatient administration service. However, the presence of allowable modifiers and payer-specific indicators means reimbursement can still shift based on configuration, especially across Medicaid plans. This highlights that while the code itself is simple, payer policy and fee schedules ultimately determine the final allowed amount, not just the CPT definition.
CMS Payment Percentage for 90471
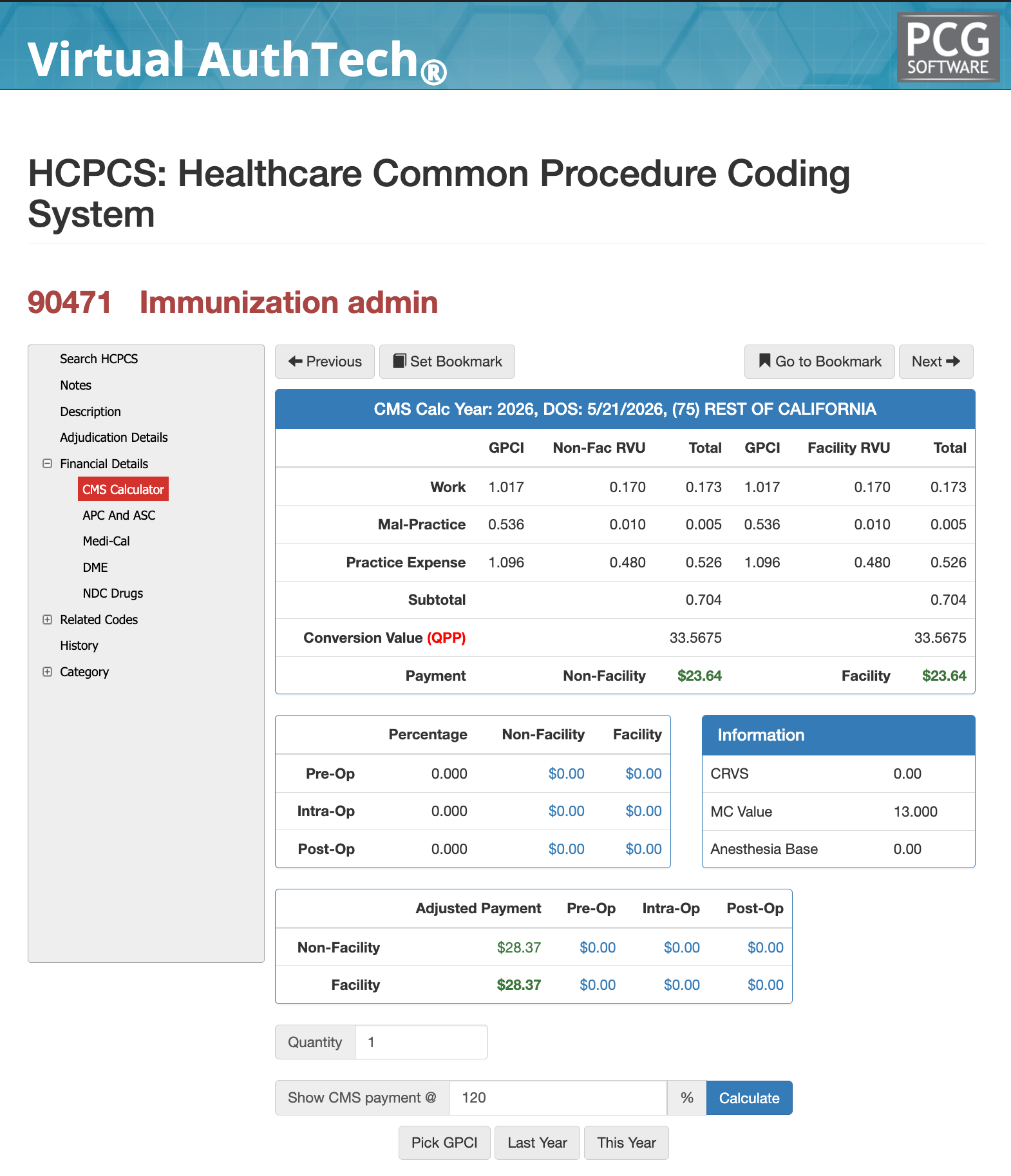
The CMS calculation for CPT 90471 is driven by its RVU components—work (0.170), malpractice (0.010), and practice expense (0.480)—which are adjusted by GPCI and multiplied by the conversion factor (~33.56), resulting in a baseline Medicare payment of about $23.64. Most payer contracts reimburse this code at 100%–120% of Medicare, meaning expected payment ranges from roughly $23.64 to $28.37 per administration, depending on the agreed percentage. Because these values shift by geography through GPCI and by contract terms, tools like iVECoder and Virtual AuthTech® allow you to model reimbursement in real time, validate expected payment at different percentage levels, and compare against your contracted rates to identify underpayments or optimization opportunities before the claim is finalized.
Common Denial Reasons for 90471
A common denial occurs when 90471 is billed alongside another administration code that should be primary, such as billing 90471 instead of 90473 (oral/intranasal) or failing to sequence add-on codes (90472) correctly. In these cases, the claim is rejected due to improper code hierarchy or incorrect route of administration.
Another frequent denial happens when 90471 is billed more than once on the same date of service, exceeding the MUE of 1. Payers expect 90471 to represent the first injection only, with additional injections billed using 90472, so duplicate primary codes are typically denied as duplicates or medically unlikely.
A third denial scenario is when 90471 is billed without a corresponding vaccine product code or with an invalid pairing, which breaks the clinical logic of the claim. Since administration must tie directly to a specific vaccine, missing or mismatched CPT/HCPCS vaccine codes will trigger denials for incomplete or unsupported services.
Are you tired or "searching online" for CPTs?
If you’ve made it this far, you’re already operating at a higher level than most clinicians, coders, and claims teams—and that’s exactly the point. You shouldn’t have to rely on memory or dig through long CPT articles every time a code like 90471 shows up. iVECoder® gives providers a fast, stand-alone way to validate coding logic, modifiers, documentation, and billing relationships in seconds, eliminating preventable denials before the claim ever goes out.
For payer organizations, Virtual Examiner® (VE) takes it further by applying that same logic across your entire claims environment—identifying overpayments, flagging FWA patterns, enforcing compliance, and automating what would otherwise take teams hundreds of hours to review manually. Virtual AuthTech® is already built into that ecosystem, giving your teams real-time coding clarity upstream as well.
At some point, continuing to rely on manual review is the real risk. If you’re ready to move from reactive coding fixes to automated accuracy and payment integrity, this is the transition point.
Click below to access iVECoder® ($99/month) or submit the form for a free payer audit with Virtual Examiner®.
About PCG
For more than 30 years, PCG Software has helped health plans, provider organizations, and delegated entities improve coding accuracy, payment integrity, compliance, and fraud, waste, and abuse detection through payer-focused software and claims auditing expertise.
Click to share with others